
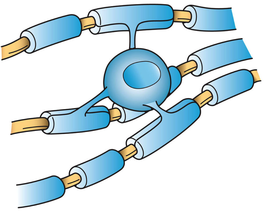
 Image 1. | The amount of white matter we have in our brains is vital to proper brain function. The substance that makes up white matter is a fatty protein called myelin. The fat component is what gives myelin it's white appearance. In the brain this substance is created by specialized cells called oligodendrocytes (image 1). They have multiple projections or arms that wrap around nerve axons to insulate them. The presence of this insulating layer is essential for nerve conduction. Normally a nerve impulse travels down an axon in a wave. In the prescence of myelin sheaths the impulse jumps and moves exponentially faster. |
| Without this myelin layer nerves don't communicate with one another properly. Image 2 shows an unmyelinated neuron on the left and a myelinated neuron on the right. It depicts how more rapidly an impulse moves when the neuron is myelinated. White matter is most dense in the interior of the brain as seen in Image 3. The gray matter on the cortex or outer shell of the brain is darker because that's were the cell bodies of most neurons exist. The nucleus and other cell organelles are found in the cell body, giving the darker appearnace. In addition, cell bodies are not myelinated. The cell bodies of the neurons in Image 2 are at the top. |  Image 2. |
 Image 3. | A new study, published this week in Neuron, reveals changes in early development and differentiation of these oligodendrocytes that make myelin. They also found actual hypomyelination if Ts65Dn mice (genetically modified to model Down syndrome in humans). Many researchers speculate that changes in brain development in utero are the root of cognition changes later in life for individuals with T21. |
One thing many researchers fail to acknowledge when studying Down syndrome is that they may actually be seeing the effects of hypothyroidism and not the over-expression of chromosome 21. Hypothyroidism is more common in children with T21 than is reported. Most doctors only check TSH (thyroid stimulating hormone) and free T4 (thyroxine). The process of thyroid hormone within the body is much more complicated than that and only testing these two lab values misses a lot of hypothyroidism. In addition, many doctors accept a TSH higher than 3, 4 and even 6 or 7 mIU/L to be normal for individuals with Down syndrome. An optimal TSH is closest to 1.5 mIU/L (1) and ideally it should be below 2.5 mIU/L. The most detrimental aspect of hypothyroidism being missed in individuals with Down syndrome is the dismissive attitudes of many doctors accepting the obvious symptoms of hypothyroidism (2) as typical for Down syndrome. For a more indepth explanation of this I recommend reading Thyroid and the Developing Brain.
The role that active thyroid hormone (triiodothyronine) plays in myelin formation, oligodendrocyte differentiation and function is strong. A study from 1997 stated, "Our results indicate that thyroid hormones participate in the control of the progenitor cell proliferation and differentiation as well as in oligodendrocyte maturation and that these two T3-regulated events are independent." (3) An even older study from 1985 also emphasized a direct effect of T3 on myelination. (4) The impact of thyroid hormone on myelination has been known for a long time. Yet, funding for research, as is often the case, is focused on finding new drugs to help those who are impacted by demyelinating disease like Multiple Sclerosis or Down syndrome.
Fortunately, more recent published information exists supporting the importance of thyroid hormone on the developing brain. A current, very comprehensive overview of this was written by Juan Bernal, M.D, Ph. D. and is called Thyroid Hormones in Development and Function. Image 4 below comes from the new study published in Neuron revealing the decrease in neuron connections in individuals with Down syndrome. The same lack of neuron connections in hypothyroidism can be seen in Image 5 from Dr. Bernal's review.
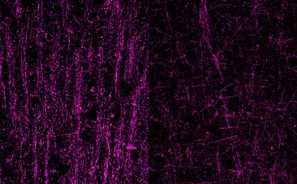 Image 4. Fluorescent images of nerve connections in the brain of a typically-developing individual, left, compared to a person with Down syndrome. (Yale University) | 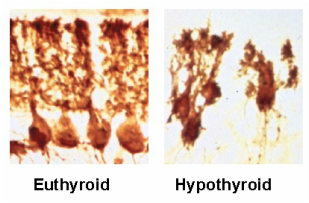 Image 5. |
Michelle Diament suggests the potential use of myelin-regenerating drugs for those with Down syndrome as a means to counter the imapct that demyelination can have in her article for Disability Scoop (5). I recommend uncovering the root cause of demyelination, dysfuntional oligodendrocyte differentiation and decreased neuron connection before using pharmaceuticals that can potentially have significant side effects, including:
- Fatigue
- Flu-like symptoms
- Depression and mood changes
- Gastrointestinal problems (6)
The key to optimizing myelination and early brain development is optimizing this process in utero. More research is needed to understand the role that thyroid hormone plays in early brain development in infants with Down syndrome and how to optimize it. Optimizing thyroid hormone in adults is potentialy as important as optimizing it in early development. Remaud, et al wrote Thyroid Hormone Signaling and Adult Neurogenesis in Mammals. They give a vast amount of evidence supporting the importance of optimal thyroid hormone function in all stages of life. As well, myelination has been reported to continue well into adolescence. (7)
There's support for other means of optimizing myelination than just ensuring proper thyroid hormone function. B12 and folate are critical for early brain development and myelination formation in utero. (8) Most importantly, however, is iron. Todrich, et all have stated, "The importance of iron in myelin production has been demonstrated by studies showing that decreased availability of iron in the diet is associated with hypomyelination. " (9) Radlowski and Johnson stated, "...the need and usage of iron by oligodendrocytes does not end during the perinatal period and that the adult brain still requires adequate iron." (10) Iron levels are commonly low in children with Down sydrome. (11, 12)
There's support for other means of optimizing myelination than just ensuring proper thyroid hormone function. B12 and folate are critical for early brain development and myelination formation in utero. (8) Most importantly, however, is iron. Todrich, et all have stated, "The importance of iron in myelin production has been demonstrated by studies showing that decreased availability of iron in the diet is associated with hypomyelination. " (9) Radlowski and Johnson stated, "...the need and usage of iron by oligodendrocytes does not end during the perinatal period and that the adult brain still requires adequate iron." (10) Iron levels are commonly low in children with Down sydrome. (11, 12)
Choline is another key nutrient needed for myelination and has been shown to be effective for remyelination. (13) Barbara Strupp's important work reveals that prenatal choline supplementation "markedly improved spatial cognition" in Ts65Dn mice. (14) One published report of a 2.5 year old boy with Down syndrome revealed "definitive" improvement in his speech and language skills in addition to his gross motor skills after supplementation with phosphatidylcholine. (15) The important role that phosphatidylcholine plays in myelin formation is most likely a mechanism that supported cogniton in these two examples.
I suggest that any research that intends to study the impact that the over-expression of chromosome 21 has on any areas of brain function including myelination remove the variables that hypothyroidism and nutrient deficiencies can have on these processes. If your child or loved one is taking any or all of these nutrients and has had early treatment for hypothyroidism it's possible that this new information about hypomyelination does not apply to them. The use of pharmaceuticals to treat myelination issues in children with Down syndrome should be approached cautiously given the many other ways that myelination can be supported.

 RSS Feed
RSS Feed