
 | I really miss teaching Cell Biology to college students. It gave me great satisfaction to teach them about the amazing machinery that exists within their bodies. My passion for this subject was evident in my lectures. I'm writing this blog post to help parents understand this subject that is so often mentioned online. I will explain here normal mitochondrial physiology then discuss mitochondrial dysfunction arising from vitamin deficiencies and biochemical disturbances that can interfere with their function. I will not be discussing genetic defects in mitochondrial DNA that impact how they function as this is a whole topic unto itself. |
Basic Mitochondrial Function
Mitochondria are small organelles that exist within cells. The number of mitochondria in cells varies greatly throughout the body. Some cell types can have as many as 1,000 - 2,000 mitochondria per cell. Located on the multiple folds of the inner membrane as well as within the fluid spaces of mitochondria are enzymes that convert breakdown products from glucose into energy.
To say that mitochondria are important to human health is grossly understating their role in our survival. We literally would not be alive without them. They're fascinating organelles that convert our food into energy so that every other function of our body can occur. Basic mitochondrial function is typically taught based on how glucose is used to make energy, but proteins and fats are used to make energy as well.
To really break it down, this whole process is really all about moving electrons. Electrons are the energy of life. They're considered subatomic particles, but they have no matter or substance to them; they're made up of nothing but energy. Every chemical process that occurs in your body happens because electrons and the energy from them are transferred to enable these processes to occur.
The terms "reduction" and "oxidation" should be explained here as they describe how electrons are transferred. Reduction occurs when a compound gains an electron, which gives the compound more negative charge, basically "reducing" it's charge. Oxidation occurs when a compound loses an electron. This term is used for this process because oxygen is the most common electron "thief" within the body.
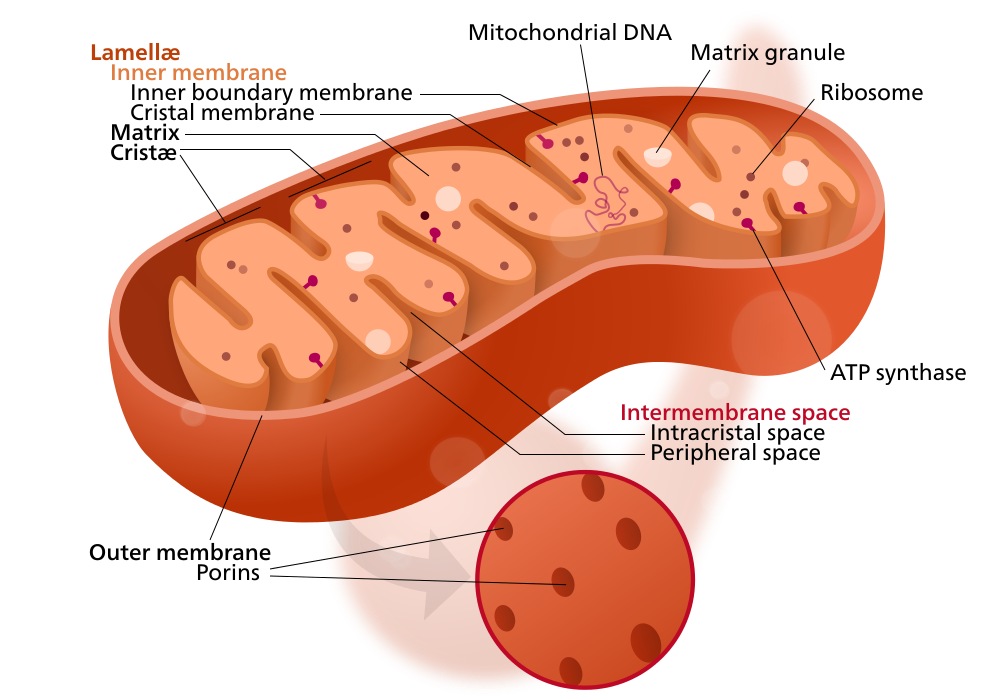
Electrons are typically carried and transferred from a high energy compound called ATP (image 1). ATP carries energy between its highly energized phosphate groups (yellow). You can see in the image that they are all negatively charged. They really don't want to be next to each other (recall that positive and negative charges attract one another and negative charges typically repel each other). Their negative charges come from an extra electron that they are carrying. It's these electrons that are transferred in order to give energy to millions of chemical processes within our body. When ATP releases one of these phosphate groups to a reaction it causes that reaction to move forward.
To say that mitochondria are important to human health is grossly understating their role in our survival. We literally would not be alive without them. They're fascinating organelles that convert our food into energy so that every other function of our body can occur. Basic mitochondrial function is typically taught based on how glucose is used to make energy, but proteins and fats are used to make energy as well.
To really break it down, this whole process is really all about moving electrons. Electrons are the energy of life. They're considered subatomic particles, but they have no matter or substance to them; they're made up of nothing but energy. Every chemical process that occurs in your body happens because electrons and the energy from them are transferred to enable these processes to occur.
The terms "reduction" and "oxidation" should be explained here as they describe how electrons are transferred. Reduction occurs when a compound gains an electron, which gives the compound more negative charge, basically "reducing" it's charge. Oxidation occurs when a compound loses an electron. This term is used for this process because oxygen is the most common electron "thief" within the body.
Electrons are typically carried and transferred from a high energy compound called ATP (image 1). ATP carries energy between its highly energized phosphate groups (yellow). You can see in the image that they are all negatively charged. They really don't want to be next to each other (recall that positive and negative charges attract one another and negative charges typically repel each other). Their negative charges come from an extra electron that they are carrying. It's these electrons that are transferred in order to give energy to millions of chemical processes within our body. When ATP releases one of these phosphate groups to a reaction it causes that reaction to move forward.
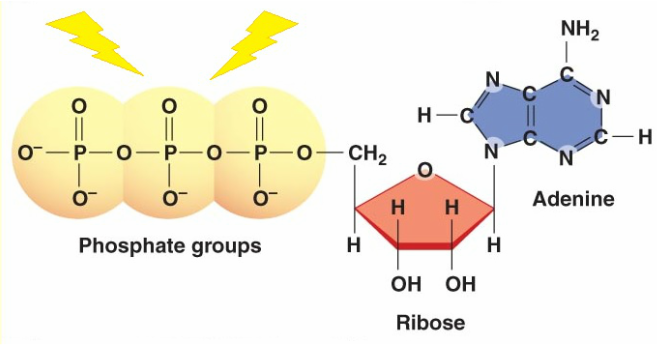
Image 1. ATP
Glycolysis, the break down of glucose to form pyruvate, is also called "harvesting of electrons". These electrons have to be handled and carried very carefully by the body so that none escape from this system. Electrons that escape create free radicals that damage cell membranes and DNA.
ATP is used to drive almost every chemical reaction within our bodies. It can also be used for something mechanical within your body like the movement of myosin heads in muscles (aka, the power stroke) along actin filaments to create a muscle contraction and relaxation as seen in the video below.
The process by which mitochondria make energy in the form of ATP is complicated but can be broken down into four basic steps:
I will focus on the steps that occur within the mitochondria only. Those are the Citric Acid Cycle and the Electron Transport Chain. These last two steps can only occur in the presence of sufficient amounts of oxygen. When oxygen levels are low, like in sleep apnea or during times of intense exercise when oxygen demand from muscles exceeds available oxygen, pyruvate cannot be shuttled into the mitochondria. Lactic acid fermentation is used instead which is much less efficient and generates only two ATP molecules.
The following video reviews the basic steps in the Citric Acid Cycle. Keep in mind, this is a basic representation and there are many other factors that are involved. You should also know that ubiquinone is CoQ10.
- Glycolysis
- Pyruvate Oxidation
- Citric Acid Cycle (Krebs Cycle or Tricarboxylic Acid Cycle - TCA)
- Electron Transport Chain (Oxidative Phosphorylation)
I will focus on the steps that occur within the mitochondria only. Those are the Citric Acid Cycle and the Electron Transport Chain. These last two steps can only occur in the presence of sufficient amounts of oxygen. When oxygen levels are low, like in sleep apnea or during times of intense exercise when oxygen demand from muscles exceeds available oxygen, pyruvate cannot be shuttled into the mitochondria. Lactic acid fermentation is used instead which is much less efficient and generates only two ATP molecules.
The following video reviews the basic steps in the Citric Acid Cycle. Keep in mind, this is a basic representation and there are many other factors that are involved. You should also know that ubiquinone is CoQ10.
The NADH and FADH2 that are generated from the TCA carry their electrons to the electron transport chain where they are used in the final step to make energy as shown in the video below. Check out that cool ATP synthase complex at the end....like mini turbines in every cell!
All of these processes work together in what's called "Cellular Respiration", so named because it's how our cells use oxygen (image 2).
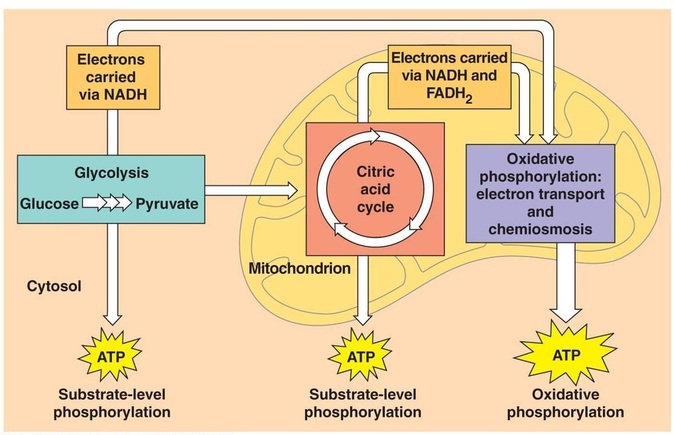
Image 2. Cellular Respiration
I made this "puzzle" years ago to use for my students (image 3) and still have it on my bookshelf. I used to have them print it, cut out all of the parts and put it together at home. They would receive an extra point on their exam if they sent me a photo of it assembled. Typically the students who found it fun and helpful really didn't need the extra point on their exam.
Image 3. Cellular Respiration puzzle
It's easy to see here how our bodies work like well-oiled machines when provided with everything it needs to function properly. For every one molecule of glucose the body is able to make approximately 35 molecules of ATP: two from glycolysis, one from the TCA and 32 from the electron transport chain. Sometimes it makes less when this process isn't working as efficiently.
If you're craving even more information on this topic, this chapter of the The Cell by Alberts B, Johnson A, Lewis J, et al. outlines these processes in much greater detail: The Mitochondrion.
The areas of highest mitochondrial activity, based on the rate of ubiquinone reduction and oxidation, are the heart, kidney and liver (1). As well, because the brain is the most metabolically active organ in the body it is vulnerable to disruptions in mitochondrial function.
If you're craving even more information on this topic, this chapter of the The Cell by Alberts B, Johnson A, Lewis J, et al. outlines these processes in much greater detail: The Mitochondrion.
The areas of highest mitochondrial activity, based on the rate of ubiquinone reduction and oxidation, are the heart, kidney and liver (1). As well, because the brain is the most metabolically active organ in the body it is vulnerable to disruptions in mitochondrial function.
Symptoms of Mitochondrial Dysfunction
Most conventional medical doctors are not trained to recognize mitochondrial dysfunction. Research supporting mitochondrial dysfunction as a clinical entity is vast and growing. However, as is often the case, much of this research is not incorporated into every day medical practice.
Several researchers have reported a connection between mitochondrial dysfunction and autism (2,3,4). In addition, mitochondrial dysfunction in Down syndrome has been well-established (5). Many biomedical clinicians have already come to accept that mitochondrial dysfunction is something to look for and treat in children with autism and other special needs. As well, many parents are seeing notable improvements in their children's health and development when mitochondria dysfunction is detected and addressed.
Because so many organs and processes of the body are dependent on ATP and the mitochondria that makes it, symptoms can be vague and impact many organ systems. These symptoms include:
You can see how easily a doctor might dismiss these symptoms as Chronic Fatigue Syndrome, Irritable Bowel Syndrome or no diagnosis is made and "there's nothing that can be done". Many times pharmaceutical drugs will be used that mask these symptoms yet never really help the patient nor address the root cause of the patient's problem.
Several researchers have reported a connection between mitochondrial dysfunction and autism (2,3,4). In addition, mitochondrial dysfunction in Down syndrome has been well-established (5). Many biomedical clinicians have already come to accept that mitochondrial dysfunction is something to look for and treat in children with autism and other special needs. As well, many parents are seeing notable improvements in their children's health and development when mitochondria dysfunction is detected and addressed.
Because so many organs and processes of the body are dependent on ATP and the mitochondria that makes it, symptoms can be vague and impact many organ systems. These symptoms include:
- Low muscle tone
- Difficulty swallowing
- Failure to thrive
- Learning disability
- Fatigue
- Delayed gut motility
- Heat/cold intolerance
- Migraines
- Lactic acidosis
- Liver disease
- Immune system problems
- Heart problems
- Kidney problems
- Neurological problems
- Autonomic dysfunction
You can see how easily a doctor might dismiss these symptoms as Chronic Fatigue Syndrome, Irritable Bowel Syndrome or no diagnosis is made and "there's nothing that can be done". Many times pharmaceutical drugs will be used that mask these symptoms yet never really help the patient nor address the root cause of the patient's problem.
What do mitochondria need in order to function properly?
All of the above steps don't just magically happen. Each of the steps requires an enzyme to make it happen and those enzymes have cofactors that are required in order for them to work. In addition, nutrients don't just automatically cross into the mitochondria; some are shuttled in with carriers.
Compounds they require to function properly:
All of the above steps don't just magically happen. Each of the steps requires an enzyme to make it happen and those enzymes have cofactors that are required in order for them to work. In addition, nutrients don't just automatically cross into the mitochondria; some are shuttled in with carriers.
Compounds they require to function properly:
- CoQ10
- B Vitamins
- L-Carnitine
- D-ribose
- Iron
- Alpha lipoic acid (6)
- Thyroid hormone (T3 and T2)
CoQ10 is a fat soluble substance; hence its position within the inner cell membrane of the mitochondria. It has three reduced states:
Ubiquinone is typically used as a supplement when mitochondria support is the goal. Ubiquininol can be used as an antioxidant because it carries two electrons that can be used to limit the damage caused by reactive oxygen species (ROS). ROS create damage because they have an unpaired electron that is seeking to be matched with another electron. This extra electron can be gained from lipids within the body or from DNA, which damages these structures. Ultimately antioxidants are electron donors and ubiquinol is one of many electron donors that serve as antioxidants. The role of CoQ10 within the mitochondria is as an elecron carrier, so ubiquinone is best. CoQ10 has been shown to lower levels of oxidized purines, which are the damaged pieces of DNA that occur as a result of oxidative stress, in cells of those with Down syndrome (7).
B vitamins are needed as enzyme cofactors for each step of the TCA and within the electron transport chain (image 4). These B vitamins can quickly become depleted in a diet that contains processed grains because those grains provide glucose but are stripped of the bran and germ that contain B vitamins to help our bodies get energy from the glucose. Deficiencies in B vitamins are also very common in those who have an imbalance in their gut flora like small intestinal bacterial overgrowth (SIBO) or candida overgrowth (8).
- Ubiquinone - fully oxidized, missing both electrons it's capable of carrying
- Semiquinone - missing one electron
- Ubiquinol - fully reduced, carrying both electrons it can can carry
Ubiquinone is typically used as a supplement when mitochondria support is the goal. Ubiquininol can be used as an antioxidant because it carries two electrons that can be used to limit the damage caused by reactive oxygen species (ROS). ROS create damage because they have an unpaired electron that is seeking to be matched with another electron. This extra electron can be gained from lipids within the body or from DNA, which damages these structures. Ultimately antioxidants are electron donors and ubiquinol is one of many electron donors that serve as antioxidants. The role of CoQ10 within the mitochondria is as an elecron carrier, so ubiquinone is best. CoQ10 has been shown to lower levels of oxidized purines, which are the damaged pieces of DNA that occur as a result of oxidative stress, in cells of those with Down syndrome (7).
B vitamins are needed as enzyme cofactors for each step of the TCA and within the electron transport chain (image 4). These B vitamins can quickly become depleted in a diet that contains processed grains because those grains provide glucose but are stripped of the bran and germ that contain B vitamins to help our bodies get energy from the glucose. Deficiencies in B vitamins are also very common in those who have an imbalance in their gut flora like small intestinal bacterial overgrowth (SIBO) or candida overgrowth (8).
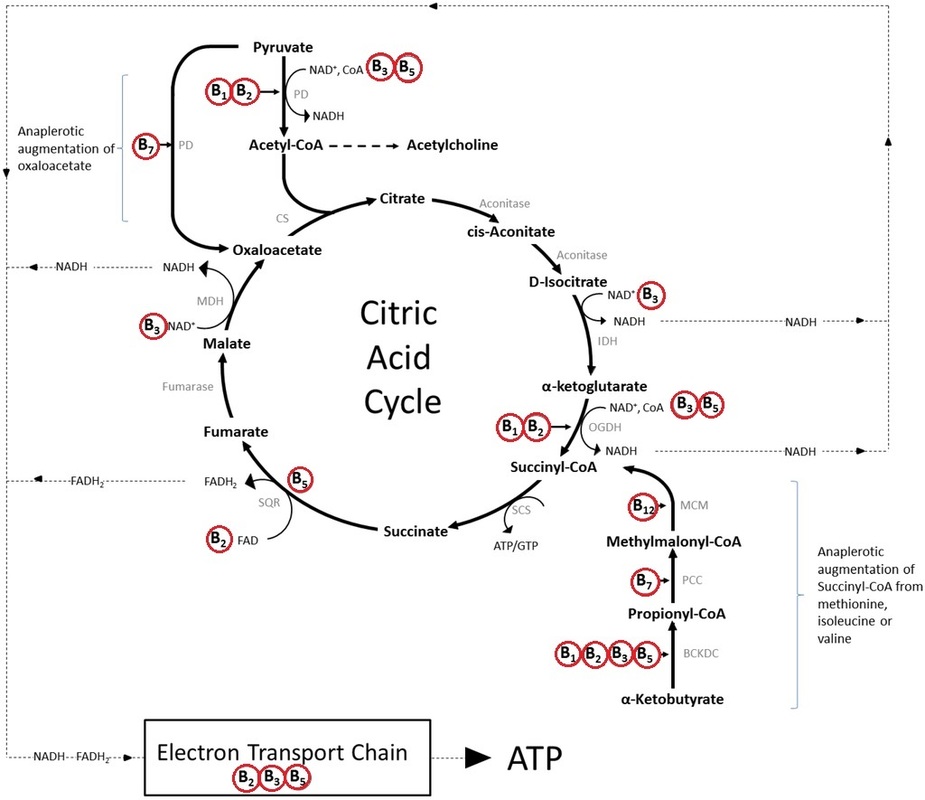
Image 4. B vitamin cofactors of the TCA
Carnitine has one role in the body and that is to shuttle fatty acids into the mitochondria so that they can be used for energy. That's it. It does nothing else. Carnitine is synthesized in the body from lysine and methionine. It's also obtained through eating meat, especially red meat, hence it's name (carne = meat). In 2005 researchers tested carnitine's impact on mitochondria function in aging rats. They found that it improved the function of the TCA and the flow of electrons through the electron transport chain (9). In addition, children with Down syndrome have been shown to have lower carnitine levels than typical children (10). Because mitochondrial function has been linked to cognition (11) it follows that carnitine supplementation can help dementia and cognitive impairment that is linked to mitochondrial dysfunction. In fact, researchers in the UK found that acetyl l-carnitine did improve cognition in those with mild cognitive impairment and mild Alzheimer's disease (12). Acetyl l-carnitine is the form of carnitine that crosses the blood brain barrier, so it's preferred when support of cognition is the goal.
Lastly, carnitine deficiency has been shown to cause delayed gut motility leading to vomitting after meals, oral drooling, delayed gastric emptying and constipation (13). This makes sense given how much muscle function is impacted by mitochondria function and optimal gut motility is a consequence of healthy muscle function.
Lastly, carnitine deficiency has been shown to cause delayed gut motility leading to vomitting after meals, oral drooling, delayed gastric emptying and constipation (13). This makes sense given how much muscle function is impacted by mitochondria function and optimal gut motility is a consequence of healthy muscle function.
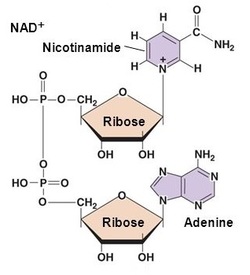 Image 5. Ribose as component of NAD+ | Ribose is a five-carbon sugar that is made in the body from glucose. It's a component of ATP and NADH/NAD+. Image 1 (above) shows ribose as a part of ATP. You can see in image 5 how NAD+ requires two ribose molecules. A recent mouse study found that ribose increased gut motility and improved their resistance to weight gain through improved energy homeostasis (14). Supplementing with D-ribose has also been shown to be helpful for chronic fatigue and fibromyalgia patients through it's ability to increase cellular energy (15). Moreover, ribose may provide protection to cells during states of elevated oxidative stress, which children with autism and Down syndrome experience (16). Because muscle tone and function is so dependent on mitochondrial function and ATP many studies exist supporting ribose's role in muscle energetics (17). |
Iron deficiency is the most common nutrient deficiency worldwide. One of the main symptoms of iron deficiency is fatigue. This is, in part, due to iron's role as a cofactor in several enzymes found within the TCA as well as the electron transport chain.
Alpha lipoic acid (ALA) is a fatty acid that is synthesized within mitochondria and acts as a very potent antioxidant. It can also be obtained in the diet in the form of lipoyllysine and is highest in animal tissue (kidney, heart, liver) and green plants like spinach and broccoli (18). In addition to being an antioxidant ALA is also required as a cofactor for one of the enzyme complexes that makes up pyruvate dehydrogenase. This enzyme complex converts pyruvate (made from glucose) to acetyl-CoA that is the entrance point for the TCA. It's thought that ALA deficiency doesn't exist as the body typically makes what it needs. However, supplementing with ALA has been shown to support brain health, cardiovascular health, heavy metal chelation, insulin function and inflammation (19, 20). It's repeatedly been shown to work well when supplemented together with acetyl l-carnitine (21,22, 23, 24).
Alpha lipoic acid (ALA) is a fatty acid that is synthesized within mitochondria and acts as a very potent antioxidant. It can also be obtained in the diet in the form of lipoyllysine and is highest in animal tissue (kidney, heart, liver) and green plants like spinach and broccoli (18). In addition to being an antioxidant ALA is also required as a cofactor for one of the enzyme complexes that makes up pyruvate dehydrogenase. This enzyme complex converts pyruvate (made from glucose) to acetyl-CoA that is the entrance point for the TCA. It's thought that ALA deficiency doesn't exist as the body typically makes what it needs. However, supplementing with ALA has been shown to support brain health, cardiovascular health, heavy metal chelation, insulin function and inflammation (19, 20). It's repeatedly been shown to work well when supplemented together with acetyl l-carnitine (21,22, 23, 24).
Thyroid hormone is often overlooked for it's vital role in mitchondrial function. There are several forms of thyroid hormone, thyroxine (T4), triiodothyronine (T3), 3,5 diiodo-l-thyronine (T2) and monoiodothyronine (T1). Each of these forms are named based on the number of iodine atoms attached to them. The two forms that play an important role in mitochondria function are T3 and T2. T3 is often called "active" thyroid hormone because it's necessary for the function of every cell within the body. T3 acts as a transcription factor within the cell, literally turning on certain genes within the nucleus of each cell that contribute to the function of that cell. T3 and T2 hormone work in a similar manner within the mitochondria; they turn on mitochondrial genes that code for key proteins with the electron transport chain (image 6).
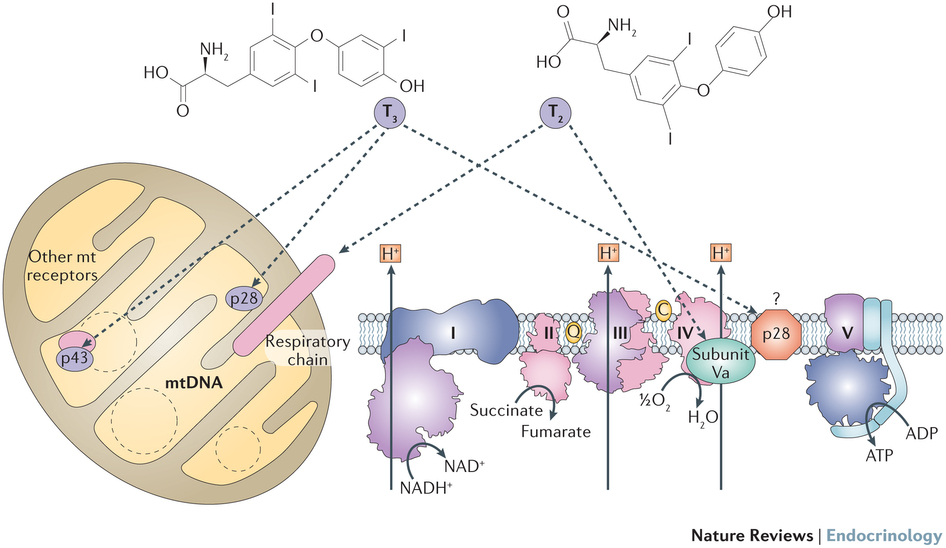
Image 6. Mechanisms of direct actions of iodothyronines T3 and T2 on mitochondria. (source: http://www.nature.com/nrendo/journal/v12/n2/fig_tab/nrendo.2015.205_F3.html)
The enzymes that convert T4 to T3 and T2 by removing an iodine molecule are deiodinase enzymes. These enzymes are selenium dependent and sensitive to several biochemical imbalances within the body including low iron, cortisol excess or deficiency, inflammation and oxidative stress. Subclinical hypothyroidism, defined as a low T4:T3 ratio has been shown to negatively impact mitochondria function (25). Thyroid hormone not only supports mitchondria function, it also has "profound effect on mitochondria biogenesis", the production of new mitochondria (26). When assessing mitochondrial function physicians need to run in-depth thyroid labs (TSH, free T4, free T3, reverse T3) and carefully review them, keeping in mind optimal levels as the goal.
Tests for Mitochondrial Dysfunction
The good news is that mitochondrial function can be assessed through blood and urine tests as well as symptoms. These tests include:
Not all doctors will order these tests, nor will they know how to interpret them. It's important to work with a doctor who has training or is educated to understand these tests. Interpreting these labs is both simple yet complicated. For example, if carnitine levels are low supplementation is warranted. Other markers that indicate a need for carnitine are urinary fatty acids, adipic and suberic acid. When they are elevated in the urine it indicates that they are not being shuttled into mitochondria and not being used, hence the need for carnitine. Doses recommended are in the range of 20-100 mg/kg/day for children (28). Elevated urinary pyruvic acid can indicate a need for alpha lipoic acid as well as B1, B2 and B3. Elevated intermediates of the TCA in the urine can indicate a need for cofactors of the enzyme needed to convert that intermediate to the next step of the TCA, typically these are B vitamins. This information is greatly simplified and assessment of what each patient needs to support their individual mitochondrial needs requires an evaluation from a trained physician.
- Plasma free carnitine and acylcarnitine
- Urine organic acid test (TCA cycle intermediates, lactic acid, pyruvic acid, ketone and fatty acid oxidation, 3-methylglutaric, 3-hydroxyglutaric, 3-methylglutaconic)
- Plasma amino acids, alanine:lysine ratio or elevated alanine (27)
Not all doctors will order these tests, nor will they know how to interpret them. It's important to work with a doctor who has training or is educated to understand these tests. Interpreting these labs is both simple yet complicated. For example, if carnitine levels are low supplementation is warranted. Other markers that indicate a need for carnitine are urinary fatty acids, adipic and suberic acid. When they are elevated in the urine it indicates that they are not being shuttled into mitochondria and not being used, hence the need for carnitine. Doses recommended are in the range of 20-100 mg/kg/day for children (28). Elevated urinary pyruvic acid can indicate a need for alpha lipoic acid as well as B1, B2 and B3. Elevated intermediates of the TCA in the urine can indicate a need for cofactors of the enzyme needed to convert that intermediate to the next step of the TCA, typically these are B vitamins. This information is greatly simplified and assessment of what each patient needs to support their individual mitochondrial needs requires an evaluation from a trained physician.
Case Report
I reported on the outcome of helping a 14 month old boy with Down syndrome in my blog post Customized Treatment for Children with Down Syndrome. His initial organic acid test results indicated significant mitochondrial dysfunction with several elevations in his TCA intermediates as well as very high adipic and suberic acid levels, indicating a need for carnitine. He was only supplemented with carnitine and treated for gastrointestinal dysbiosis, which was the greatest contributing factor to his B vitamin deficiencies. His repeat organic acid results as well as his improved development and cognition indicated that mitochondria function had improved.
Summary
Many children with special needs (Down syndrome, autism, and others) would benefit from screening for mitochondrial dysfunction. The long term impact to health and cognition if mitochondrial dysfunction goes unaddressed are profound. The benefits of supporting mitochondrial function are far-reaching for the patient given the many organ systems that are impacted by cellular energy production.
Mitocondrial dysfuntion is currently not recognized by conventional medical physicians who often choose to prescribe pharmaceuticals for symptoms in lieu of addressing the root cause of disease. Fortunately physicians who are trained in mitochdondrial function exist and include Functional Medicine practitioners, Naturopathic physicians, Biomedical doctors and MAPS doctors.
Mitocondrial dysfuntion is currently not recognized by conventional medical physicians who often choose to prescribe pharmaceuticals for symptoms in lieu of addressing the root cause of disease. Fortunately physicians who are trained in mitochdondrial function exist and include Functional Medicine practitioners, Naturopathic physicians, Biomedical doctors and MAPS doctors.
References
- Aberg F., Appelkvist E.L., Dallner G., Ernster L. Distribution and redox state of ubiquinones in rat and human tissues. Arch. Biochem. Biophys. 1992;295:230–234.
- Palmieri L, Persico AM. Mitochondrial dysfunction in autism spectrum disorders: cause or effect?Biochim Biophys Acta. 2010;1797(6–7):1130–7.
- Rossignol DA, Frye RE. Mitochondrial dysfunction in autism spectrum disorders: a systematic review and meta-analysis. Mol Psychiatry 2012; 17: 290–314.
- Rossignol DA, Frye RE. Mitochondrial dysfunction in autism spectrum disorders: a systematic review and meta-analysis. Mol Psychiatry. 2012;17(3):290–314.
- Helguera P, Seiglie J, Rodriguez J, Hanna M, Helguera G, Busciglio J. Adaptive Downregulation of Mitochondrial Function in Down Syndrome. Cell metabolism. 2013;17(1):132-140.
- Nicolson GL. Mitochondrial dysfunction and chronic disease: treatment with natural supplements. Altern Ther Health Med. 2013
- Tiano L., Busciglio J. Mitochondrial dysfunction and Down’s syndrome: is there a role for coenzyme Q10? BioFactors. 2011;37(5):386–392.
- Dibaise, JK. Nutritional Consequences of Small Intestinal Bacterial Overgrowth. Nutrition Issues in Gastroeneterology. December 2008.
- Kumaran S, Subathra M, Balu M, Panneerselvam C. Supplementation of L-carnitine improves mitochondrial enzymes in heart and skeletal muscle of aged rats. Experimental Aging Research.2005;31(1):55–67.
- Seven M, Cengiz M, Tüzgen S, Iscan MY. Plasma carnitine levels in children with Down syndrome.Am J Hum Biol. 2001 Nov–Dec;13(6):721–5.
- Picard M, McEwen BS. Mitochondria impact brain function and cognition.Proceedings of the National Academy of Sciences of the United States of America. 2014;111(1):7-8.
- Montgomery S., Thal L., Amrein R. Meta-analysis of double blind randomized controlled clinical trials of acetyl-L-carnitine versus placebo in the treatment of mild cognitive impairment and mild Alzheimer’s disease. Int. Clin. Psychopharmacol. 2003;18:61–71.
- Weaver LT, Rosenthal SR, Gladstone W, Winter HS. Carnitine deficiency: a possible cause of gastrointestinal dysmotility. Acta Paediatr. 1992 Jan;81(1):79-81.
- Liu Y, Li T-RR, Xu C, Xu T. Ribose Accelerates Gut Motility and Suppresses Mouse Body Weight Gaining. International Journal of Biological Sciences. 2016;12(6):701-709.
- Teitelbaum J. E., Johnson C., St. Cyr J. The use of D-ribose in chronic fatigue syndrome and fibromyalgia: a pilot study. Journal of Alternative and Complementary Medicine. 2006;12(9):857–862.
- Addis P, Shecterle LM, Alexander J. Cellular protection during oxidative stress: A potential role for d-ribose and antioxidants. J Diet Suppl. 2012, 9 (3).178-82.
- Dodd SL, Johnson CA, Fernholz K, St Cyr JA. The role of ribose in human skeletal muscle metabolism.Medical hypotheses. 2004;62:819–24.
- Lodge JK, Youn HD, Handelman GJ, et al. Natural sources of lipoic acid: determination of lipoyllysine released from protease-digested tissues by high performance liquid chromatography incorporating electrochemical detection. J Appl Nutr. 1997;49(1 & 2):3-11.
- Shay KP, Moreau RF, Smith EJ, Smith AR, Hagen TM. Alpha-lipoic acid as a dietary supplement: Molecular mechanisms and therapeutic potential.Biochimica et biophysica acta. 2009;1790(10):1149-1160.
- Gomes MB, Negrato CA. Alpha-lipoic acid as a pleiotropic compound with potential therapeutic use in diabetes and other chronic diseases. Diabetology & Metabolic Syndrome. 2014;6:80.
- McMackin CJ, Widlansky ME, Hamburg NM, et al. Effect of Combined Treatment with Alpha Lipoic Acid and Acetyl-L-Carnitine on Vascular Function and Blood Pressure in Coronary Artery Disease Patients. Journal of clinical hypertension (Greenwich, Conn). 2007;9(4):249-255.
- Zhang H, Jia H, Liu J, et al. Combined R-α–lipoic acid and acetyl-L-carnitine exerts efficient preventative effects in a cellular model of Parkinson’s disease.Journal of Cellular and Molecular Medicine. 2010;14(1-2):215-225.
- Kumaran S, Savitha S, Anusuya Devi M, Panneerselvam C. L-carnitine and DL-α-lipoic acid reverse the age-related deficit in glutathione redox state in skeletal muscle and heart tissues. Mechanisms of Ageing and Development. 2004;125(7):507–512.
- Soczynska JK, Kennedy SH, Chow CS, Woldeyohannes HO, Konarski JZ, McIntyre RS. Acetyl-L-carnitine and alpha-lipoic acid: possible neurotherapeutic agents for mood disorders? Expert Opin Investig Drugs. 2008;17(6):827–843.
- Kvetny J, Wilms L, Pedersen PL, Larsen J. Subclinical hypothyroidism affects mitochondrial function.Hormone and Metabolic Research. 2010;42(5):324–327.
- Wrutniak-Cabello C., Casas F., Cabello G. Thyroid hormone action in mitochondria. J. Mol. Endocrinol.2001;26:67–77.
- Haas RH, Parikh S, Falk MJ, et al. The In-Depth Evaluation of Suspected Mitochondrial Disease: The Mitochondrial Medicine Society’s Committee on Diagnosis. Molecular genetics and metabolism. 2008;94(1):16-37.
- Parikh S, Saneto R, Falk MJ, et al. A Modern Approach to the Treatment of Mitochondrial Disease. Current treatment options in neurology. 2009;11(6):414-430.

 RSS Feed
RSS Feed